Coronary artery disease caused by calcium buildup represents one of the most complex challenges in modern cardiology, demanding innovative solutions beyond traditional treatment methods. When fatty deposits and minerals accumulate within coronary arteries, they can harden into calcified plaques that resist standard intervention techniques. Malaysian cardiologists, led by consultant cardiologist Datuk Dr Tamil Selvan Muthusamy, are now conducting research into a novel device that may offer patients with severely calcified arteries a more effective treatment pathway that could reduce complications and improve long-term outcomes.
Arterial plaque develops gradually over years as a mixture of fat, cholesterol, calcium, cellular debris and fibrin accumulates along artery walls. This buildup progressively narrows blood vessels, restricting blood flow and depriving tissues of vital oxygen. When left untreated, the condition can trigger life-threatening complications including heart attacks, heart failure and strokes. The severity of the disease typically depends on both the extent of blockage and the composition of the plaque itself. Soft, lipid-rich plaques respond well to conventional treatment, but calcium-heavy deposits present fundamentally different obstacles that require specialized approaches.
Conventional treatments for coronary artery disease include lifestyle modifications, pharmaceutical interventions and several surgical procedures designed to restore blood flow. Percutaneous coronary intervention (PCI), coronary artery bypass grafting (CABG) and angioplasty have proven effective for many patients. In standard cases, cardiologists insert a balloon catheter to compress soft plaque against artery walls, creating space for a stent that maintains the vessel's open structure. This approach fails dramatically when confronted with severe calcification, where the hardened deposits resist mechanical compression and may damage the balloon or equipment before any therapeutic effect occurs.
When extensive calcium deposits are present, conventional angioplasty becomes extraordinarily difficult and often ineffective. The rigidity of calcified plaque prevents the balloon from expanding adequately, making stent placement problematic and leaving the artery vulnerable to restenosis, or renarrowing. Alternative techniques including rotational atherectomy and high-pressure balloon angioplasty offer some benefit but carry substantial risks and frequently deliver suboptimal results. These limitations have prompted cardiologists worldwide to explore fundamentally different technologies capable of breaking down calcium deposits while preserving surrounding tissue integrity.
Intravascular lithotripsy (IVL) emerged as a breakthrough technology addressing this clinical challenge. The procedure uses sonic pressure waves generated by a catheter to fracture hardened plaque deposits within blood vessels. Instead of mechanical crushing or thermal ablation, acoustic energy creates controlled fracture patterns that crack calcified material into smaller fragments, allowing the artery to expand naturally. Despite its innovative approach, conventional IVL systems have inherent constraints limiting their clinical utility. The technology depends on external energy generators with fixed pulse numbers, typically ranging from eight to twelve pulses per procedure.
Dr Tamil Selvan explains the fundamental limitation of conventional IVL systems: the number of acoustic pulses available must be rationed across the entire treatment zone. If a calcified blockage spans a significant distance, clinicians may exhaust their pulse allocation before achieving complete plaque disruption. Additionally, the bulky catheter design struggles to navigate through severely narrowed vessels where residual luminal space is minimal. The standardized balloon sizing presents another constraint, as coronary arteries vary significantly in diameter along their length. A three-millimetre balloon cannot accommodate vessels that expand to 3.5 or 4 millimetres proximally before tapering to 2 millimetres distally, forcing clinicians to employ multiple balloons or complementary techniques.
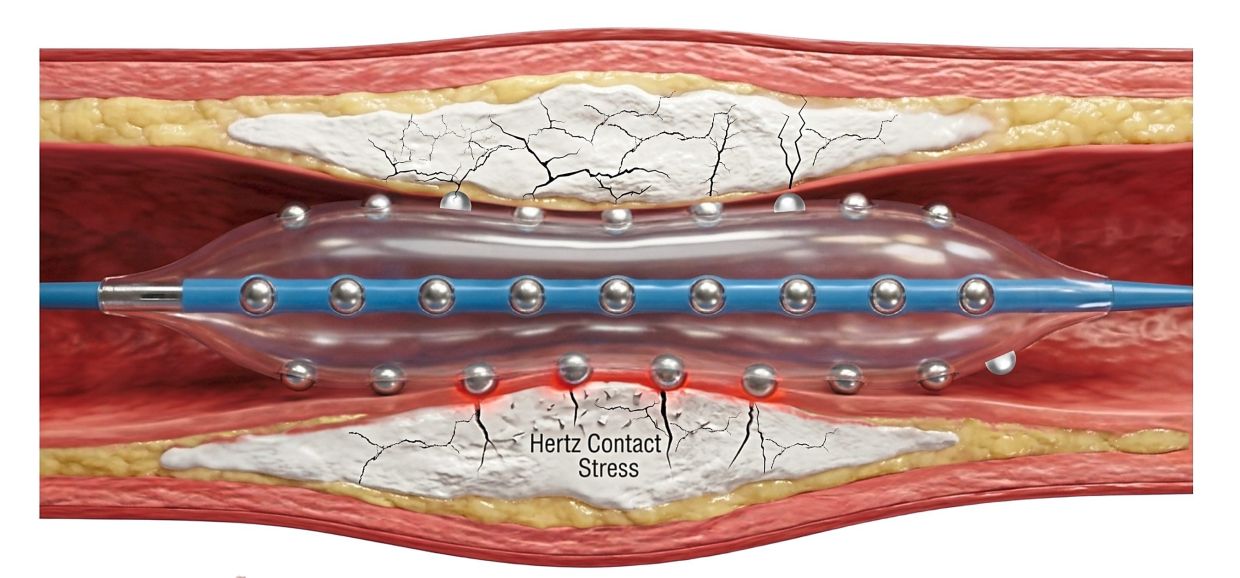
Recognizing these limitations, researchers have developed the Hertz Contact-IVL System (HC-IVL), a mechanically-based alternative to energy-dependent lithotripsy devices. Rather than relying on external ultrasound generators, the HC-IVL integrates tiny stainless steel hemispheres into the balloon itself. When the balloon contacts hardened plaque under applied pressure, the hemispheres amplify and concentrate force at the plaque surface, creating deep fracture patterns without damaging vessel walls or surrounding tissue. This mechanical approach fundamentally eliminates the pulse limitation inherent in conventional IVL systems, allowing treatment of lengthy lesions and multiple blockages with a single balloon. The improved deliverability means the catheter can navigate through the entire coronary tree more readily, significantly enhancing procedural flexibility.
Dr Tamil Selvan emphasizes the mechanical advantage of the new system: rather than applying external energy, pressure is generated and concentrated through the hemispherical contact points. When the operator applies force to the balloon, that pressure gets multiplied and transmitted to the plaque surface with tremendous intensity, creating the acoustic effect necessary to fracture calcium deposits. The system's superior trackability through narrow and calcified vessels reduces procedural complexity and shortens intervention times. Perhaps most importantly, the HC-IVL approach generates deep, extensive cracks in calcified plaque that promote optimal arterial recoil and stent expansion, potentially improving both immediate procedural success and long-term patency rates.
The international developer of HC-IVL had conducted limited feasibility studies across multiple United States centres, demonstrating the device's basic safety and functionality. However, these early investigations involved small patient populations, leaving significant gaps in understanding the technology's performance across diverse patient populations and complex anatomical presentations. Dr Tamil Selvan and his Malaysian cardiology colleagues recognized an opportunity to advance the scientific evidence base by conducting a more comprehensive, locally-based study. This research initiative reflects Malaysia's growing capacity to lead clinical research in specialized cardiology and contribute meaningfully to international knowledge regarding advanced interventional techniques.
The Malaysian study team's decision to expand upon international data demonstrates how regional cardiology programmes can play crucial roles in validating emerging technologies for specific populations. Malaysian patient populations may exhibit different demographic characteristics, disease severity patterns, comorbidity profiles and genetic factors that influence device performance. By conducting rigorous local research, the team ensures that evidence supporting HC-IVL adoption incorporates data reflecting the actual patient populations who will ultimately receive treatment. This approach strengthens the scientific foundation for implementing the technology regionally and contributes valuable information to the global cardiology community.
The implications of successful HC-IVL validation extend beyond individual patients to reshape regional cardiovascular care delivery systems. Currently, patients with severely calcified coronary artery disease in Malaysia and neighbouring countries face limited definitive treatment options, often requiring complex multi-stage procedures or surgery when conventional intervention fails. An effective, minimally-invasive technology offering superior outcomes would substantially reduce procedural complications, hospitalisation duration and healthcare costs while improving patient quality of life. For healthcare systems across Southeast Asia managing increasing coronary artery disease burdens driven by urbanisation and lifestyle changes, the HC-IVL system represents a potential game-changer in treating complex, calcified disease that previously offered few satisfactory solutions.

